
 Socio-Economics and Health
Socio-Economics and Health
 Ringkasan Isi Sesi
Ringkasan Isi Sesi
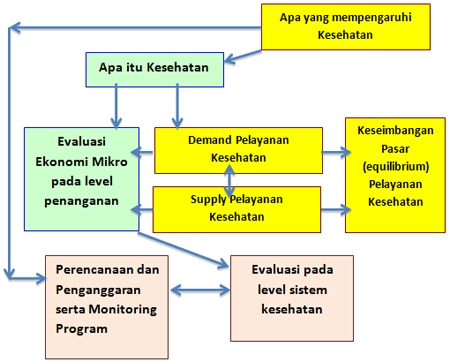
Sesi ini membahas berbagai aspek sosial yang berada di pinggiran ilmu ekonomi kesehatan. Aspek sosial ini menyangkut berbagai hal terkait dengan Social Determinant dari kesehatan. Satu aspek sosial yang mempengaruhi kesehatan adalah aspek akses masyarakat terhadap pelayanan kesehatan. Dari 6 pembicara (abstrak terlampir) masalah akses dibahas oleh Trisnantoro dalam konteks sejarah. Pada intinya masyarakat yang berada di daerah remote kurang akses dibanding dengan di daerah non-remote yang dapat membahayakan tercapainya tujuan Universal Coverage. Akses geografis ini dapat memburuk apabila tidak ada perhatian pemerintah untuk melakukan penyeimbangan. Apabila diserahkan kepilihan hidup dokter maka akan sulit terjadi pemerataan. Dokter cenderung senang bekerja di daerah maju. Secara sosial kultural faktor dokter menjadi isu penting untuk keberhasilan universal coverage.
Sementara itu ada masalah akses budaya seperti yang ditulis oleh Rebecca Reeve mengenai lebih banyaknya suku Aborigin yang sakit di daerah non-remote NSW Australia karena masalah akses terhadap pelayanan primer. Aspek pendapatan bukan menjadi faktor penting untuk menerangkan mengapa ada kesenjangan diabetes antara kelompok Aborigin dan non-aborigin. Perbedaan dalam masalah kegemukan dan pendidikan yang merupakan proksi untuk akses terhadap pelayanan kesehatan dan perilaku baik karena pendidikan terlihat menjadi pendorong terjadinya kesenjangan tersebut. Laki-laki aborigin terlihat cenderung under-diagnosed karena kekurangan akses ke pelayanan kesehatan primer. Implikasinya adalah bahwa intervensi yang mengarah kekegemukan, latihan fisik, peningkatan pengetahuan dan akses ke pelayanan kesehatan primer akan menghasilkan manfaat untuk mengurangi diabetes. Hasil ini penting untuk pengambil kebijakan walupun masih diperlukan riset dengan data.
Karina Wibowo seorang mahasiswa PhD di Jerman yang berdarah Indonesia meneliti mengenai diskrimasi yang dirasakan oleh warga pendatang di Jerman. Disebutkan bahwa pendatang merasakan adanya diskriminasi dari sistem kesehatan di Jerman. Hal serupa dirasakan oleh orangtua walaupun merasa puas dengan pelayanan kesehatan. Terakhir orang tua dari etnis tertentu merasa kurang puas dan merasa didiskriminasi dalam pelayanan kesehatan. Hasil ini menunjukkan bahwa dalam aspek sosial ada "sesuatu" yang dirasakan tidak berjalan baik dalam pelayanan kesehatan. "Sesuatu" ini menyangkut hal yang abstrak yang dalam penelitian ini berusaha diungkapkan.
Tiga pembicara lain membahas mengenai berbagai aspek sosial yang mempengaruhi asthma dan hipertensi, serta pengaruh kematian anak dalam fertilitas. John Gibson (University of Waikato. Faculty of Economics) membandingkan pendatang Tonga yang datang ke New Zealand melalui lotere dibandingkan dengan yang gagal mendapatkan di Tonga. Berbeda dengan harapan, hasilnya menunjukan bahwa migrasi dari Tonga ke New Zealand menunjukkan perbaikan kinerja baru. Salah satu penyebab mengapa terjadi karena perubahan lingkungan social yang mengurangi merokok di kelompok migran laki-laki. Kawan diyono dari Survei Meter meneliti mengenai hipertensi dan persamaan dan perbedaan antara situasi di Indonesia dengan hasil-hasil dari berbagai studi di negara lain. Dengan penelitian ini diharapkan dapat membuat para pakar kesehatan masyarakat mengembangkan intervensi dan program yang spesifik untuk masyarakat Indonesia pada umumnya dan kelompok-kelompok masyarakat . Marwân-al-Qays Bousmah dari Aix-Marseille School of Economics Perancis meneliti mengenai hubungan antara kematian anak dan perilaku peningkatan fertilitas. Implikasi kebijakan adalah bersamaan dengan perbaikan status kesehatan dan perkembangan kelangsungan hidup anak, kebijakan-kebijakan kesehatan yang bertujuan untuk mengurangi kematian anak akan mempunyai dampak pada perilaku fertilitas. Kebijakan-kebijakan ini akan bersifat mendukung trasisi fertilitas secara sukarela dengan cepat di negara-negara Sub-Sahara Afrika, bersamaan dengan program keluarga berencana tradisional.
Penulis: Laksono Trisnantoro
Silahkan melihat abstraknya di bawah ini:
ABSTRAK 1: Can Indonesia improve socio-economic and geographic equity together? A historical analysis
Presenter: Laksono Trisnantoro (Gadjah Mada University. Faculty of Culture)
Background: In Indonesia, the effort for achieving universal coverage will have new momentum in 2014. However the past experience of Indonesian health service system shows that increasing the coverage of health protection scheme is not a simple policy. This research provides historical facts, which have influenced health equity in Indonesia and discuss a possible dilemma in reducing economic and geographical inequity at present and in the future. Method: Historical analysis. Results: As a direct response to the economic crisis in the late 1990's, financial protection for health care for the poor was set nationally in 1999. The protection policy aimed to reduce out of pocket spending by increasing central government funding targeting the poor. A steady growth of central government funding for health social security resulted in a relatively low incidence of catastrophic out of pocket health expenditure, which has declined over time. The financial protection program reduced financial barriers to access for poor households for both hospital and non-hospital services. However, alongside these positive impacts, the regional inequalities in access to services have not improved over time. There is regional inequity due to shortages and mal-distribution of inputs such as health facilities, medical specialist and trained nurses. Historical facts will be used to explain this situation. Indonesia has taken the route of market –based economies and is has not been a welfare state since the colonial era. Hospitals and health service providers are distributed based on market demands and cluster in the cities and regions with good economic development. Conclusion: The new Law faces a difficult challenge in terms of geographic inequity. The geographic problems have deep roots in Indonesian health system development. There is a possibility that the improvement of socio-economic equity may worsen the geographic inequity in Indonesia.
Key Terms: geographical inequity, universal coverage, and history of health service
Authors (2): Baha'uddin (GadjahMada University. Faculty of Culture) and Laksono Trisnantoro (Faculty of Medicine, GadjahMada University. Center for Health Service Management)
ABSTRAK 2: What factors drive the gap in diabetes rates between Aboriginal and non-Aboriginal people in non-remote New South Wales?
Presenter: Rebecca Reeve (University of Technology-Sydney. Centre for Health Economics Research and Evaluation)
Background and Objective: Despite established risk factors for type 2 diabetes in the general population, there is limited research on the size and significance of these risk factors in Australian Aboriginal populations, particularly in non-remote areas. In New South Wales (NSW), 95 per cent of the Aboriginal population live in non-remote areas. The objective of this study was to identify the factors underpinning the growing gap in diabetes rates between Aboriginal and non-Aboriginal people in NSW. The results indicate the most appropriate target areas for policy interventions, which can be used as indicators to monitor progress towards reducing the gap. Methods: Data from the 2004-05 National Health Survey (NHS) and National Aboriginal and Torres Strait Islander Health Survey (NATSIHS) were used to estimate the differences between Aboriginal and non-Aboriginal people in NSW in terms of self-reported diabetes rates and risk/prevention factors. Logistic regression models were used to investigate the contribution of each factor to predicting the probability of diabetes. The analysis was restricted to non-remote areas due to ABS restrictions on the use of geographic variables, which prevent the identification of remote areas by state. Results: In non-remote NSW, risk factors for diabetes are more prevalent in the Aboriginal sample and prevalence of diabetes is 2.5 to 4 times higher in Aboriginal compared to non-Aboriginal adults. The odds of (known) diabetes for Aboriginal and non-Aboriginal Australians, in non-remote locations, are significantly higher for older people, those with low levels of school education and those who are overweight or obese. After controlling for other risk and prevention factors, low income is only associated with increased risk of diabetes in the non-Aboriginal sample. In the Aboriginal sample, the odds of diabetes are significantly higher for people reporting high levels of psychological distress. Males only have higher odds of known diabetes in the non-Aboriginal sample. Conclusions: Income does not appear to be important in explaining the gap in rates of diabetes between Aboriginal and non-Aboriginal people living in non-remote NSW. Differences in BMI and education (a proxy for ability to access and act upon health knowledge) appear to be driving the gap in diabetes rates. Psychological distress may also contribute to increased risk of diabetes in the Aboriginal population. Aboriginal men may be more likely to be under-diagnosed due to lack of access to primary care services. Implications The evidence suggests that interventions targeting obesity, exercise, improving knowledge and access to primary care services will have the greatest potential benefit for reducing the diabetes gap. The results are useful for policy makers as they show that current strategies appear to be appropriately aligned with the evidence. However, further research using longitudinal data is required to determine whether the specific methods being used to achieve these targets are effective.
Biographical Details:
Rebecca Reeve is a team investigator on CHERE's NHMRC Capacity Building grant and is program manager of the CHERE's policy evaluation program of research. She also manages the cost-effectiveness study of Drug and Alcohol Consultation Liaison Services in NSW hospitals, commissioned by NSW Health. Rebecca has an Honours degree in Economics (2004) and a PhD in Economics (Macquarie University 2010). In 2011, she received a UTS Faculty of Business grant to investigate the factors underpinning the growing gap between Aboriginal and non-Aboriginal diabetes rates in New South Wales, which is the topic of her iHEA presentation.
Key Terms: Aboriginal, diabetes, risk factors, non-remote NSW
Authors (5):Rebecca Reeve (University of Technology, Sydney. Centre for Health Economics Research and Evaluation) , Jody Church (University of Technology, Sydney. Centre for Health Economics Research and Evaluation) , Marion Haas (University of Technology, Sydney. Centre for Health Economics Research and Evaluation) , Wylie Bradford (Macquarie University. Economics) and Rosalie Viney (University of Technology, Sydney. Centre for Health Economics Research and Evaluation)
ABSTRAK 3: Immigration and Respiratory Health: Experimental Evidence from a Migration Lottery
Presenter: John Gibson (University of Waikato. Economics)
Theme: Application
Respiratory disorders such as asthma and chronic obstructive pulmonary disease (COPD) are the fourth leading cause of death worldwide. While asthma is a reversible inflammatory disorder of the airways, which especially affects children, COPD is non-reversible and especially affects the elderly. The main causes of COPD are smoking in rich countries and indoor cooking smoke in poor countries. There is debate about causes of asthma, which almost doubled in some rich countries over the past 25 years. In New Zealand, which is the context for this research, the burden of asthma and COPD is second only to cardiovascular diseases, in terms of disability-adjusted life years. New Zealand has one of the highest asthma rates in the world, with substantial ethnic inequality. Maori and Pacific children have higher prevalence and hospitalization rates for asthma than do children of other ethnic groups and the highest rate of increase in asthma over the last two decades was for Pacific Island children [ISAAC: International Study of Asthma and Allergies in Childhood]. The burden of respiratory illnesses for Maori and Pacific Islanders reflects higher smoking rates, poor housing with substantial overcrowding and possibly the unequal impacts of air pollution. Immigrants are of special significance in the literature on asthma since migration involves exposure to a new set of pollutants and allergens and also affects housing conditions, all which have possible links with asthma. This literature finds that the foreign-born arriving from countries with lower asthma prevalence experience a time-dependent increase in asthma symptoms. Comparisons between foreign-born and native-born survey respondents suffer from two potential problems: selection bias and reporting bias. Selection bias may mask the true extent of the migration-dependent increase in asthma if immigrants are more or less asthma-prone than non-migrants from their home country. Reporting bias may occur because of changes in access to health care with migration, with respondents only becoming aware of long-standing health disorders if they have improved access to health care after migrating. To overcome these problems, this paper uses a natural experiment, comparing successful and unsuccessful applicants to a migration lottery to experimentally estimate the impact of migration on self reported asthma and measured respiratory functioning. Approximately four years after migration we compare migrants who had entered New Zealand through a random ballot with unsuccessful participants in the same ballots living in the home country of Tonga. Contrary to expectations, the results show migration from Tonga to New Zealand to improve lung functioning, as measured by peak flow. The rate of moderate asthma indicated by peak flow as a percentage of the expected peak flow adjusted for age, gender and height, falls by between 10 to 20 percentage points. One possible cause of this improved respiratory health is a substantial decline in current smoking amongst immigrant males. This experimental evidence indicates that there is no inevitable decline in respiratory health following migration from a low-asthma to a high-asthma environment and raises questions about whether findings in the existing literature have been affected by self-selection and reporting biases.
Key Terms: Respiratory health, Immigration, Natural experiment
Authors (4): John Gibson (University of Waikato. Economics) , Steven Stillman (University of Otago. Economics) ,HalahinganoRohorua (University of Waikato. Economics) and David McKenzie (World Bank. Development Research Group)
ABSTRAK 4: Assessing Social Determinants as Predictors to Conversion to Hypertension: Evidence from the Indonesia Family Life Survey (IFLS)
Presenter: KawandiyonoSantoso (SurveyMETER)
Hypertension is a leading risk factor to global mortality. Though silent and chronic, it is not unpreventable. Designing preventive public health interventions should start with identifying characteristics associated with becoming hypertensive. Our research used the longitudinal Indonesia Family Life Survey (IFLS) to investigate the contribution of a full range of potential determinants (i.e., demographic, socio-economic, behavioral, psychological, and health systesms) known from research on other populations to be associated with hypertension. Using the IFLS, we tracked blood pressure measurements on a panel, nationally representative sample of 10,846 adults who in 1997 had normal blood pressure and who stated on interview they had never been told they have high blood pressure. Using blood pressure measurements and self-reports in 1997 and two subsequent survey rounds, we categorized each person as either having converted or not converted to high blood pressure by 2007. Twenty-nine percent of our sample converted to hypertensive status in that ten years period. Using information about individual and community characteristics from the IFLS 1997, we used logistic regression to determine which characteristics, observable prior to conversion to high blood pressure status, were associated with that conversion. We will report on results of this analysis, including gender, geographic and socio-economic differences in these predictors. These results will shed light on similarities and differences between Indonesia and results from studies in other countries, allowing public health professionals to tailor interventions and programs specific to the Indonesian context and to specific sub-populations within Indonesia.
Key Terms: social determinants, predictor, hypertension
Authors (2): KawandiyonoSantoso (SurveyMETER) and Jeffrey Sine (RTI International. Social Political Health Economic Research)
ABSTRAK 5: Evidence for a Non-Linear Effect of Child Mortality on Fertility Behaviors: Micro Data from a Senegalese Rural Community
Presenter: Marwân-al-QaysBousmah (Aix-Marseille University, CNRS & EHESS. GREQAM)
The present paper seeks to take the analysis of the relationship between child mortality and fertility behaviors one step further by highlighting a new link between these two variables. In particular, it reconciles the ongoing debate between the 'child survival hypothesis' and the 'replacement hypothesis', as both strategies can be prominent depending on the burden of child mortality. We use individual data collected quarterly within the Demographic Surveillance System of the rural community of Niakhar (Fatick, Senegal), which is Africa's oldest statistical observatory. We analyze the complete birth histories of 2884 women born between 1931 and 1962, which are typical count data. The determinants of fertility are investigated using a standard Poisson Regression Model. Several spécifications are estimated to emphasize the heterogeneous effects of child mortality on both total and net fertility. Among them, fractional polynomial transformations of the child mortality variable are used in order to capture the potential non-linear nature of the relationship. In line with other empirical studies,the global impact of child mortality on total and net fertility is found to be positive. More precisely, we find that women who have experienced at least one child death have a total fertility, which is 1.47 higher than women who have not. Such an increase is proved to be larger than the one needed to replace lost lives, as net fertility is also 1.12 higher. We further show that the response is non linear in the level and in the rate of child mortality, as the amplitude and the direction of the effect vary with the number of child losses. To our knowlegde, this is the first paper to provide evidence that the 'child survival hypothesis' and the 'replacement hypothesis' are not mutually exclusive. A precautionary demand for children is likely to arise for relatively low values of child mortality. However, when child deaths increase, a replacement mechanism prevails. Finally, for dramatic values of child mortality, the rise in total fertility does not fully compensate for child losses, so that net fertility falls. The results hold when we account for the effect of child mortality in level or in rate, and are robust to changes in econometric specifications. The main policy implication is that, along with health outcomes and child survival improvements, health policies aiming at reducing child mortality have additional desirable effects on fertility behaviors. These policies are likely to be supportive of a rapid and voluntary fertility transition in Sub Saharan Africa along with traditional family planning programs.
Authors (2): Marwân-al-QaysBousmah (Aix-Marseille University (Aix-Marseille School of Economics), CNRS & EHESS. GREQAM) and Mohammad Abu-Zaineh (INSERM? Aix-Marseille University (Aix-Marseille School of Economics). SESSTIM)
ABSTRAK 6: How satisfied are migrants and the elderly in the German health care? A case study on Germany of perceived racism and ageism in the German health care
Presenter: Karina Wibowo (Jacobs University & University of Bremen. Bremen International Graduate School of Social Sciences)
Our population is undergoing an inevitable phenomenon of aging due to the demographic transition. Such change makes it necessary to get more people to fill the job vacancies. As a result, an increasing number of workers need to be hired from abroad. Such influx of foreign population is a normal outcome of the demographic transition which could have been foreseen. However the society has not been prepared for such changes. As minority population increases, they are easily discriminated against, especially if the outcome of the population growth is not expected (Becker, 1975). The increase of the elderly is viewed negatively by younger population. They believe such increase changes their daily life due to the adaption politically and economically since the elderly are living on the costs of the younger population. (BMBF 2012, Schmähl). Immigrants are viewed in a similar way: according to the economical active population, immigrants come to the country to live on local social welfare, which is in the end supported by the taxes of the indigenous population. Thus elderly and immigrants are seen to be a burden to the economically active population, which is comprised of the younger German population. The stereotypes towards the elderly and immigrants can result in discrimination, which has been shown by a lot of studies. Simply put: „Elderly and immigrants are allowed but they are not welcome". Therefore this study concentrates on perceived racism and ageism in the German health care among Christian communities. Christian communities were chosen since racism in Germany often occurred due to discrimination against the Islamic religion (lit). Furthermore no migrants with a Turkish background were taken into account, since numerous studies have shown that they are discriminated against. Therefore this study focuses on migrant communities other than Turkish one (lit). The hypothesis, which were tested were following: 1. Patients with an ethnic background are less satisfied with the health care and feel discriminated. 2. The elderly is less satisfied with the health care and feels discriminated. 3. The Elderly with an ethnic background are least satisfied with the health care and feel most discriminated. Methods An online survey was prepared in order to investigate in the perceived discrimination of migrants and the elderly. This survey covered questions on physician- patient relationship (including trust towards the physician, satisfaction with the physician and the medical treatment), satisfaction with the hospital (including questions on waiting hours, access to health care), perceived health behavior (healthy lifestyle), perceived health status and discrimination (observed discrimination and perceived discrimination). Results The results show that migrants perceive discrimination in the German health care system. On the other hand, the elderly are satisfied with the health care system but they perceive some level of discrimination. Finally, the elderly with an ethnic background feel less satisfied and also perceive discrimination. As the demographic transition of the society is transitioning towards more elderly and elderly with an ethnic background the problem of discrimination in the health care has to be tackled.
Key Terms: racism, ageism, patient's care, discrimination
Author (1): Karina Wibowo (Jacobs University, University of Bremen. Bremen International Graduate School of Social Sciences)





 Diskusi ini membahas tentang perkembangan menarik dalam obat. Majalah Forbes memperkirakan akan ada obat seharga jutaan dolar setahun di pasar. Isu mengerucut tentang biaya dari Orphan Drugs dan perkembangan kedokteran personal memberikan alarm untuk anggaran kesehatan di dunia.
Diskusi ini membahas tentang perkembangan menarik dalam obat. Majalah Forbes memperkirakan akan ada obat seharga jutaan dolar setahun di pasar. Isu mengerucut tentang biaya dari Orphan Drugs dan perkembangan kedokteran personal memberikan alarm untuk anggaran kesehatan di dunia.

 Deskripsi Sesi
Deskripsi Sesi Countries around the world continue to face challenges associated with rising health care expenditures and competing demands for limited resources, long wait times for care, and citizens who expect more from their health care system. In response, some countries, including Australia and Ireland, have experimented with systems of parallel private finance that offers citizens faster access to health care services for a price (including those covered through publicly-funded insurance), with suggestions by some that this can alleviate pressure on the publicly-funded system. Some single payer countries, like Canada, are facing pressure to follow suit and add a parallel private tier. What can single-payer health care systems learn from the experiences of their multi-payer counterparts? What can multi-payer health care systems learn from their single-payer counterparts? What does the research evidence say about the impact of parallel private finance on key measures like access, costs, physician behavior and citizen satisfaction? This panel of experts from Australia, Ireland, Canada, the United States, the United Kingdom and Taiwan will present the latest evidence on the positive and negative effects of parallel private finance and options for health system sustainability.
Countries around the world continue to face challenges associated with rising health care expenditures and competing demands for limited resources, long wait times for care, and citizens who expect more from their health care system. In response, some countries, including Australia and Ireland, have experimented with systems of parallel private finance that offers citizens faster access to health care services for a price (including those covered through publicly-funded insurance), with suggestions by some that this can alleviate pressure on the publicly-funded system. Some single payer countries, like Canada, are facing pressure to follow suit and add a parallel private tier. What can single-payer health care systems learn from the experiences of their multi-payer counterparts? What can multi-payer health care systems learn from their single-payer counterparts? What does the research evidence say about the impact of parallel private finance on key measures like access, costs, physician behavior and citizen satisfaction? This panel of experts from Australia, Ireland, Canada, the United States, the United Kingdom and Taiwan will present the latest evidence on the positive and negative effects of parallel private finance and options for health system sustainability.
